“What Size Kidney Cyst Is Dangerous?” Not all kidney cysts are dangerous—but size matters. Learn which cyst sizes could pose risks and when to talk to your doctor.
Understanding the Alarm Bells of Kidney Cysts

What Kidney Cysts look like
Kidney cysts affect nearly half of all people over 50 years old, making them one of the most common incidental findings during medical imaging. These fluid-filled sacs within the kidneys often cause immediate anxiety when discovered, despite the fact that most are completely harmless. However, distinguishing between benign growths and potentially dangerous lesions requires understanding critical factors beyond simple presence.
While the majority of renal cysts pose no health threat, certain characteristics—particularly size, structural complexity, and accompanying symptoms—serve as warning signals that demand immediate medical attention. Size thresholds, ranging from 3 centimeters to over 10 centimeters, help physicians determine appropriate monitoring strategies and intervention timing. Complex features such as thick walls, internal septations, calcifications, and solid components significantly elevate malignancy risk regardless of dimensions.
This comprehensive guide examines the precise size criteria that distinguish routine findings from concerning lesions, explores the internationally recognized Bosniak classification system, and provides essential information about diagnostic procedures, treatment options, and long-term prognosis. Understanding these medical principles empowers patients to make informed decisions while reducing unnecessary anxiety about common benign conditions.
Basics of Kidney Cysts
What are Kidney Cysts?

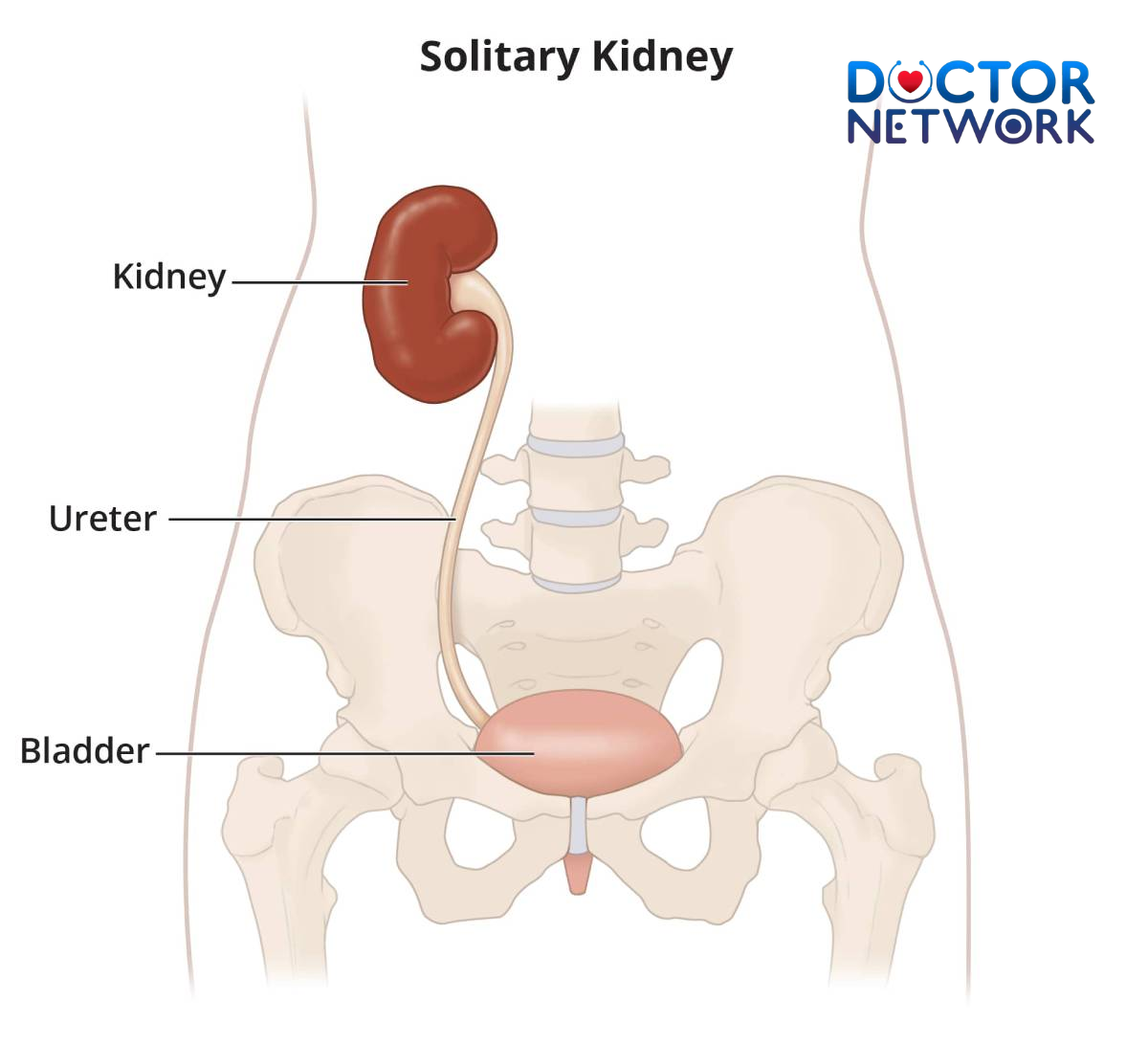
Kidney Cysts
Kidney cysts are fluid-filled sacs that develop within the renal parenchyma, typically containing clear, straw-colored liquid similar to urine. These formations occur when nephrons become blocked, causing fluid accumulation and gradual expansion over time. The prevalence increases dramatically with age, affecting approximately 25% of individuals over 40 and rising to 50% in those over 50 years old.
Most renal cysts form spontaneously without identifiable causes, though genetic factors, kidney injuries, and certain medications may contribute to their development. Unlike polycystic kidney disease (PKD), which involves multiple inherited cysts throughout both kidneys, simple kidney cysts typically appear as isolated lesions. The majority remain stable in size throughout a person’s lifetime, growing slowly at rates of 1-2 millimeters annually.
Types of Kidney Cysts: Simple vs. Complex
Simple cysts represent the most common variant, characterized by thin walls (less than 2 millimeters), round or oval shapes, and homogeneous fluid content without internal structures. These benign lesions demonstrate smooth borders on imaging studies and show no enhancement with contrast agents during CT or MRI examinations. Simple cysts carry zero malignancy risk and require no treatment unless they cause symptoms through mass effect.
Complex cysts exhibit features that distinguish them from their simple counterparts, including thick walls, internal septations, calcifications, hemorrhage, or solid components. These characteristics raise concern for potential malignancy and necessitate careful evaluation using the Bosniak classification system. Complex lesions may contain infected material, blood products, or protein deposits that alter their appearance on medical imaging.
The Bosniak Classification system serves as the primary tool for categorizing complex cysts and assessing their malignancy risk. Developed by Dr. Morton Bosniak in 1986, this internationally accepted framework helps radiologists and urologists determine appropriate management strategies based on specific imaging characteristics. The classification ranges from Category I (simple benign cysts) to Category IV (clearly malignant lesions requiring immediate surgical intervention).
When Does Kidney Cyst Size Become a Concern?

Polycystic Kidney Disease
The “Dangerous” Size Thresholds
Most simple cysts measuring under 3-4 centimeters in diameter are considered clinically insignificant and require no intervention beyond routine monitoring. These small lesions rarely cause symptoms and maintain their benign characteristics throughout patients’ lifetimes. Medical guidelines consistently recommend observation rather than active treatment for asymptomatic simple cysts in this size range.
Increased vigilance becomes necessary when cysts exceed 5 centimeters in diameter, regardless of their simple appearance on imaging studies. Larger lesions carry higher potential for symptom development, including flank pain, abdominal discomfort, and pressure sensations. Additionally, complex cysts over 5 centimeters demonstrate statistically higher malignancy rates compared to smaller complex lesions with identical Bosniak classifications.
Significant concern arises with cysts exceeding 7-10 centimeters in diameter, as these massive lesions frequently cause symptoms through compression of surrounding structures. Large cysts may compress adjacent organs, blood vessels, or the collecting system, leading to pain, hypertension, or impaired renal function. Even benign giant cysts often require surgical intervention to alleviate mass effect symptoms.
| Cyst Size | Clinical Significance | Typical Management |
|---|---|---|
| <3 cm | Usually benign, minimal concern | Routine observation |
| 3-5 cm | Low risk, monitor for growth | Annual imaging follow-up |
| 5-7 cm | Moderate concern, symptom potential | Every 6-month monitoring |
| 7-10 cm | High symptom likelihood | Consider intervention |
| >10 cm | Mass effect probable | Surgical evaluation recommended |
The crucial caveat remains that size represents only one factor among many in determining cyst significance. A small, complex cyst with solid components or thick septations poses greater malignancy risk than a large, simple cyst with thin walls and clear fluid content. Bosniak classification takes precedence over size measurements when assessing malignancy potential.
Beyond Size: Other Red Flags (Bosniak Classification Deep Dive)
Bosniak Category I encompasses simple benign cysts with hairline-thin walls, no septa, calcifications, or solid components, and water-density contents. These lesions carry 0% malignancy risk and require no follow-up imaging unless symptoms develop. Category I cysts appear as well-defined, homogeneous masses with smooth contours on all imaging modalities.
Bosniak Category II includes minimally complex cysts with thin septa (less than 1 millimeter), fine calcifications in walls or septa, or high-density contents due to hemorrhage or protein. These lesions maintain less than 1% malignancy risk and require no routine follow-up. Category II cysts may demonstrate minimal complexity but retain fundamentally benign characteristics.
Bosniak Category IIF (F for follow-up) represents indeterminate lesions requiring surveillance imaging due to minimal complexity that exceeds Category II criteria. These cysts may contain multiple thin septa, minimal smooth thickening, or small calcifications. Category IIF lesions carry 5-10% malignancy risk, necessitating imaging follow-up every 6-12 months to detect progression.
| Bosniak Category | Key Features | Malignancy Risk | Management |
|---|---|---|---|
| I | Simple, thin walls, no septa | 0% | No follow-up needed |
| II | Thin septa, fine calcifications | <1% | No follow-up needed |
| IIF | Multiple septa, minimal thickening | 5-10% | Imaging surveillance |
| III | Thick walls/septa, enhancement | 40-60% | Surgical intervention |
| IV | Solid components, clear enhancement | >90% | Immediate surgery |
Bosniak Category III designates moderately complex cysts with thick walls or septa, nodular calcifications, or heterogeneous enhancement patterns. These lesions demonstrate 40-60% malignancy risk and typically require surgical intervention or biopsy for definitive diagnosis. Category III cysts exhibit features suspicious for renal cell carcinoma and warrant urological consultation.
Bosniak Category IV identifies clearly malignant lesions with obvious solid enhancing components, thick irregular walls, or extensive nodular elements. These lesions carry greater than 90% malignancy risk and require immediate surgical management, typically involving partial or radical nephrectomy. Category IV cysts represent frank renal cell carcinomas requiring oncological treatment protocols.
Accompanying Symptoms that Signal Danger
Flank pain represents the most common symptom associated with problematic kidney cysts, typically manifesting as dull, aching discomfort in the side or back below the ribs. Pain may worsen with physical activity, certain positions, or during urination. Large cysts can compress surrounding tissues, causing chronic pain that interferes with daily activities and sleep quality.
Hematuria, or blood in the urine, serves as a critical warning sign that demands immediate medical evaluation regardless of cyst size or complexity. Microscopic hematuria may only be detectable through laboratory testing, while gross hematuria produces visible red or pink discoloration. Blood in urine may indicate cyst rupture, infection, or underlying malignancy requiring urgent investigation.
Hypertension development or worsening of existing high blood pressure may result from large cysts compressing renal blood vessels or affecting kidney function. The renin-angiotensin system becomes activated when renal perfusion decreases, leading to secondary hypertension that may be difficult to control with standard medications. New-onset hypertension in patients with large kidney cysts warrants immediate evaluation.
Additional concerning symptoms include:
- Recurrent urinary tract infections (UTIs)
- Decreased urine output or changes in urination patterns
- Abdominal swelling or palpable masses
- Unexplained weight loss or fatigue
- Persistent fever or chills
Impaired kidney function, as demonstrated by elevated serum creatinine levels or decreased glomerular filtration rate, may occur when large cysts compress normal renal tissue or obstruct the collecting system. Bilateral large cysts or numerous cysts can significantly reduce functional kidney tissue, leading to chronic kidney disease progression.
Diagnosis and Monitoring: The Role of Imaging
Initial detection of kidney cysts occurs most commonly as incidental findings during imaging studies performed for unrelated medical concerns. Abdominal CT scans, MRI examinations, and ultrasounds frequently reveal unsuspected renal lesions, leading to patient anxiety and need for further evaluation. The widespread use of medical imaging has dramatically increased the detection rate of asymptomatic kidney cysts.
Key Diagnostic Tools
Ultrasound serves as the initial screening modality for kidney cyst evaluation, offering excellent visualization of simple cysts while avoiding radiation exposure. This non-invasive technique effectively demonstrates cyst size, location, and basic characteristics such as wall thickness and internal echoes. Ultrasound readily distinguishes between simple fluid-filled cysts and more complex lesions requiring additional imaging.
Limitations of ultrasound include operator dependence, difficulty visualizing small lesions, and inability to adequately characterize complex cysts for Bosniak classification. Doppler ultrasound can detect blood flow within lesions but cannot replace cross-sectional imaging for comprehensive evaluation. Most simple cysts diagnosed by ultrasound require no further imaging unless symptoms develop.
CT scanning (Computed Tomography) provides detailed evaluation of complex cysts and remains essential for accurate Bosniak classification. Multi-phase CT examinations include pre-contrast, arterial phase, and delayed phase imaging to assess enhancement patterns within cystic lesions. Enhancement of 10-15 Hounsfield units or greater suggests solid components and raises malignancy concern.
Modern CT protocols optimize image quality while minimizing radiation exposure through dose reduction techniques and iterative reconstruction algorithms. Contrast-enhanced CT scanning can identify subtle features invisible on other imaging modalities, including thin septations, small solid nodules, and minimal wall thickening. Three-dimensional reconstructions help surgeons plan interventions when necessary.
MRI (Magnetic Resonance Imaging) offers an excellent alternative to CT scanning, particularly for patients with renal function impairment or contrast allergies. MRI provides superior soft tissue contrast and can detect enhancement without iodinated contrast agents using gadolinium-based compounds. Diffusion-weighted imaging helps distinguish between benign and malignant lesions.
Monitoring Strategy
Watchful waiting, also termed active surveillance, represents the standard approach for simple cysts and low-risk complex lesions (Bosniak II and IIF). This strategy involves regular imaging follow-up to detect growth, symptom development, or morphological changes suggesting malignant transformation. Follow-up intervals depend on initial Bosniak classification and patient-specific factors.
Surveillance protocols typically recommend imaging every 6-12 months for Bosniak IIF lesions, while simple cysts require no routine follow-up unless symptoms develop. Stable lesions over 5 years may warrant less frequent monitoring, though individual patient circumstances influence surveillance strategies. Any change in cyst characteristics necessitates prompt re-evaluation and possible intervention.
Intervention criteria include rapid growth (>50% volume increase over 6-12 months), development of complex features, symptom onset, or patient preference for definitive treatment. Large symptomatic cysts may require drainage or surgical removal regardless of benign appearance. Bosniak III and IV lesions warrant surgical consultation regardless of size or symptoms.
Treatment and Management Options
Asymptomatic benign cysts require no treatment beyond routine observation, as intervention risks outweigh potential benefits for stable, simple lesions. The vast majority of kidney cysts remain stable throughout patients’ lifetimes without causing symptoms or complications. Regular medical follow-up ensures prompt detection of any changes requiring intervention.
For Symptomatic or Concerning Cysts
Aspiration and sclerotherapy involves percutaneous drainage of cyst fluid followed by injection of sclerosing agents to prevent recurrence. This minimally invasive procedure utilizes imaging guidance to insert a needle into the cyst, aspirate contents, and inject ethanol or other sclerosants. Success rates approach 80-90% for appropriate candidates, though cyst recurrence remains possible.
Candidates for aspiration include patients with large symptomatic simple cysts who are poor surgical candidates or prefer less invasive treatment. The procedure requires local anesthesia and can be performed on an outpatient basis. Complications include pain, bleeding, infection, and potential injury to surrounding structures, though serious adverse events are rare.
Laparoscopic cyst decortication represents the gold standard surgical treatment for symptomatic kidney cysts, offering excellent success rates with minimal morbidity. This minimally invasive approach involves removal of the cyst wall accessible to the peritoneal cavity while preserving normal kidney tissue. Five small incisions allow insertion of laparoscopic instruments and a camera for precise dissection.
Advantages of laparoscopic surgery include reduced postoperative pain, shorter hospital stays, faster recovery times, and excellent cosmetic results compared to open surgical approaches. Success rates exceed 95% for appropriate cases, with very low recurrence rates. Most patients resume normal activities within 2-3 weeks following surgery.
Partial nephrectomy involves surgical removal of the cyst along with a portion of surrounding normal kidney tissue, typically reserved for complex lesions with malignancy concern. This nephron-sparing approach preserves maximum kidney function while ensuring complete lesion removal. Robotic-assisted techniques have improved precision and outcomes for partial nephrectomy procedures.
Radical nephrectomy requires complete kidney removal and is reserved for extensive malignant lesions or cases where partial nephrectomy is not technically feasible. This procedure may be necessary for large, complex cysts with definitive malignant features or when cancer has spread beyond the kidney capsule. Most patients with one healthy kidney maintain normal renal function long-term.
Managing Complications
Cyst infection requires antibiotic treatment and may necessitate percutaneous drainage for large infected collections. Infected cysts typically present with fever, flank pain, and urinary symptoms. Broad-spectrum antibiotics targeting gram-negative bacteria are usually effective, though culture-guided therapy provides optimal treatment.
Cyst rupture can cause severe pain and hematuria but rarely requires intervention unless bleeding is significant. Most ruptured cysts heal spontaneously with conservative management including pain control and monitoring. Large hemorrhages may require hospitalization and occasionally interventional radiology procedures to control bleeding.
Malignant transformation of complex cysts necessitates oncological management including staging studies, multidisciplinary team consultation, and appropriate surgical intervention. Renal cell carcinomas arising from cystic lesions generally have good prognoses when detected early and treated appropriately. Regular surveillance of complex cysts helps identify malignant changes before metastatic spread occurs.
Living with Kidney Cysts: Patient Perspective & Prognosis
Psychological Impact
The discovery of kidney cysts often triggers significant anxiety and fear, as patients may immediately associate any kidney abnormality with cancer or kidney failure. This emotional response is completely understandable and normal, especially given the vital importance of kidney function for overall health. Healthcare providers must address these concerns with clear, compassionate communication about the benign nature of most kidney cysts.
Patient education plays a crucial role in reducing anxiety and promoting informed decision-making. Understanding that kidney cysts are extremely common, affecting nearly half of all adults over 50, helps normalize the diagnosis and reduce fear. Many patients benefit from written educational materials, online resources, and support groups connecting them with others who have similar diagnoses.
The uncertainty associated with complex cysts requiring surveillance can create ongoing stress and worry between follow-up appointments. Patients may experience “scanxiety” before imaging studies, fearing progression or malignant transformation. Mental health support, including counseling or anxiety management techniques, may benefit some individuals struggling with the psychological aspects of cyst monitoring.
Long-term Outlook
Simple kidney cysts have an excellent prognosis, with the vast majority remaining stable and asymptomatic throughout patients’ lifetimes. These benign lesions do not transform into malignant tumors and rarely cause kidney function impairment or other serious complications. Most people with simple kidney cysts live completely normal lives without any impact on longevity or quality of life.
Complex cysts classified as Bosniak IIF have good long-term outcomes when properly monitored, with most remaining stable over years of surveillance. The small percentage that do progress can be detected early through regular imaging and treated effectively. Early detection and treatment of any malignant transformation result in excellent cure rates for renal cell carcinoma.
Even patients requiring surgical intervention for large symptomatic cysts or complex lesions generally have excellent outcomes with modern minimally invasive techniques. Laparoscopic procedures offer high success rates with low complication rates and quick recovery times. Most patients return to full activity within weeks of surgery with complete symptom resolution.
Kidney function typically remains normal after cyst treatment, whether through drainage procedures or surgical removal. The remaining healthy kidney tissue compensates effectively, maintaining adequate renal function for normal daily activities. Regular monitoring ensures early detection of any kidney function changes requiring medical management.
When to Seek Medical Advice
Ongoing communication with nephrologists or urologists remains essential for patients with kidney cysts, particularly those with complex lesions requiring surveillance. Regular scheduled appointments allow for symptom assessment, review of imaging results, and adjustment of monitoring protocols as needed. Patients should never hesitate to contact their healthcare providers with questions or concerns between visits.
Immediate medical attention is warranted for severe flank pain, visible blood in urine, fever with urinary symptoms, or significant changes in urination patterns. These symptoms may indicate cyst complications such as rupture, infection, or bleeding requiring urgent evaluation. Emergency department visits may be necessary for severe symptoms, especially outside normal clinic hours.
New symptoms developing between scheduled follow-up appointments should prompt earlier medical evaluation rather than waiting for the next planned visit. Changes in pain patterns, development of abdominal swelling, or new urinary symptoms may indicate cyst growth or complications requiring immediate attention. Patient awareness and prompt reporting of new symptoms optimize outcomes.
Patients should maintain detailed records of their symptoms, medications, and imaging results to facilitate communication with healthcare providers and ensure continuity of care. Regular blood pressure monitoring is particularly important for patients with large cysts, as hypertension may develop gradually and require treatment. Annual kidney function testing helps detect any subtle changes in renal performance.
Informed Vigilance
Kidney cysts represent one of the most common findings in medical imaging, affecting millions of people worldwide with the vast majority being completely benign lesions requiring no treatment. Understanding the key factors that distinguish harmless simple cysts from potentially dangerous complex lesions empowers patients to make informed decisions about their healthcare while avoiding unnecessary anxiety about common benign conditions.
Size thresholds provide important guidance, with cysts under 3-4 centimeters rarely causing concern, while those exceeding 5-7 centimeters warrant closer monitoring regardless of their simple appearance. However, the Bosniak classification system remains the most critical tool for assessing malignancy risk, with complex features such as thick walls, septations, and solid components taking precedence over size measurements in determining appropriate management strategies.
Regular medical surveillance, appropriate imaging studies, and prompt attention to new symptoms ensure optimal outcomes for all patients with kidney cysts. The combination of advancing imaging technology, minimally invasive treatment options, and improved understanding of cyst biology has dramatically improved the prognosis for patients requiring intervention while providing reassurance for those with benign lesions.
We strongly encourage patients to maintain regular medical check-ups, follow recommended surveillance protocols for complex cysts, and seek prompt consultation with qualified healthcare professionals for any concerns regarding kidney health. Open communication with nephrologists and urologists, combined with patient education and awareness, provides the foundation for excellent long-term outcomes in kidney cyst management.
Top 5 Frequently Asked Questions About “What Size of Kidney Cyst Is Dangerous”
1. What size of kidney cyst is considered dangerous?
Kidney cysts larger than 5 cm (about 2 inches) are more likely to cause symptoms or complications and are generally considered more dangerous, especially if they continue to grow or have complex features.
However, even smaller cysts (3–4 cm) with suspicious characteristics (such as thick walls or solid areas) may also require close monitoring.
2. Is the risk from a kidney cyst determined only by its size?
No, the risk is not determined by size alone. The appearance of the cyst (whether it is simple or complex), its growth rate, and whether it causes symptoms are equally important factors.
Complex cysts, regardless of size, are more likely to be dangerous or cancerous and require further evaluation.
3. Can a kidney cyst become cancerous based on its size?
The size alone does not determine if a cyst is cancerous. Most simple cysts, even large ones, are benign.
Complex cysts with irregular walls, septations, or solid components are at higher risk for malignancy, and their risk is classified using the Bosniak system (categories I to IV).
4. What complications can occur with large kidney cysts?
Large cysts (>5 cm) can cause pain, discomfort, infection, bleeding, rupture, or blockage of urine flow, potentially leading to kidney damage.
In rare cases, especially with multiple or complex cysts, kidney function can be impaired, possibly leading to kidney failure.
5. Should a kidney cyst be removed if it is larger than 5 cm?
Not always. If the cyst is simple (thin-walled, fluid-filled, no suspicious features) and not causing symptoms, it usually only requires regular monitoring.
Surgical removal or other interventions are considered if the cyst is large, symptomatic, growing rapidly, or has suspicious/complex features.
References
Stoller, M. L., & Chi, T. (2020). Smith & Tanagho’s General Urology (19th ed.). McGraw-Hill Education.
This is a foundational textbook in urology that provides clinical context for managing simple and complex renal cysts. It is not available via a single public link, but it is a standard reference in medical libraries and practices.
Marumo, K., Horiguchi, Y., Nakagawa, K., Oya, M., Ohigashi, T., & Murai, M. (2004). Natural History of Simple Renal Cysts: A Long-Term Prospective Study. The Journal of Urology, 171(4), 1401–1404.
Bosniak, M. A. (1986). The current radiological approach to renal cysts. Radiology, 158(1), 1–10.
This is the original, seminal paper that introduced the classification system.
Link: https://pubs.rsna.org/doi/10.1148/radiology.158.1.3510019
Smith, A. D., Remer, E. M., Cox, K. L., Soroush, A., Klink, J. F., Campbell, S. C., & American Urological Association. (2012). Malignancy rates in Bosniak III and IV complex renal cysts. Urology, 79(3), 663–667.
Schoots, I. G., Zaccai, K., Hunink, M. G. M., & Verhagen, P. C. M. S. (2017). Revisiting the Bosniak classification: a systematic review and meta-analysis of the diagnostic performance of CT for discriminating benign from malignant cystic renal masses. European Radiology, 27(6), 2257–2269.
Kiểm Duyệt Nội Dung
More than 10 years of marketing communications experience in the medical and health field.
Successfully deployed marketing communication activities, content development and social networking channels for hospital partners, clinics, doctors and medical professionals across the country.
More than 6 years of experience in organizing and producing leading prestigious medical programs in Vietnam, in collaboration with Ho Chi Minh City Television (HTV). Typical programs include Nhật Ký Blouse Trắng, Bác Sĩ Nói Gì, Alo Bác Sĩ Nghe, Nhật Ký Hạnh Phúc, Vui Khỏe Cùng Con, Bác Sỹ Mẹ, v.v.
Comprehensive cooperation with hundreds of hospitals and clinics, thousands of doctors and medical experts to join hands in building a medical content and service platform on the Doctor Network application.